












All posts by hochfelder
Platelet-rich plasma injections may lead to improvements in tissue healing
After platelet-rich plasma injections, researchers have described the structural change in the healing process as well as improvement in patients’ pain and function, in a new report.
Source: ScienceDaily
Arthroscopic Treatment of Hip Pain in Adolescent Patients With Borderline Dysplasia of the Hip: Minimum 2-Year Follow-Up
To examine arthroscopic treatment of hip pain in patients with borderline hip dysplasia (lateral center edge angle [LCEA] between 20° and 25°).
Source: NCBI
Total knee arthroplasty: analysis shows EXPAREL reduces length of hospital stay and improves discharge status compared to standard analgesic modality
Pacira Pharmaceuticals, Inc. has announced results of new data showing that EXPAREL® (bupivacaine liposome injectable suspension) infiltration compared to a standard analgesic regimen in patients undergoing total knee arthroplasty (TKA) significantly decreased the length of hospital stay and increased the likelihood that a patient would be discharged to their home rather than a care facility when released from the hospital.
Source: Today Topics
Outcomes of Hip Arthroscopy in Competitive Athletes.
To evaluate the minimum 2-year postoperative clinical outcomes and the rate of return to sports in athletes who underwent capsular plication for the treatment of ligamentous laxity and/or borderline dysplasia during hip arthroscopy for the treatment of femoroacetabular impingement and labral pathology.
Source: NCBI
Yogurt consumption in older Irish adults linked with better bone health
The tidiest observational part to date of dairy intakes and bone and peculiarity measurements in older grown-ups has develop that enlarged yogurt consumption was associated with a elevated hip bone density and a significantly norm down jeopardy of osteoporosis in older females and men on the ait of Ireland, after enrapturing into account familiar risk media.
Source: ufob
Intense training without proper recovery may compromise bone health in elite rowers
Bone mineral density, an indicator of bone strength, typically increases with regular exercise, acting as a protective mechanism against bone fractures and osteoporosis. But a new study suggests that the extended, high-intensity training sessions of elite athletes could reverse beneficial bone changes.
Source: ScienceDaily
What is the recovery like after a knee replacement?

Today we will answer another one of the most common questions I am asked from people considering knee replacement surgery. “How long is the recovery?” Although this is one of the most common questions we are asked, it is also one of the hardest to answer. At Hudson Valley Bone and Joint Surgeons we have replaced over 3,000 knees over the past several decades, and one thing that we know for sure is that each person recovers at their own pace. We recently performed a knee replacement on a high school gym teacher who was back to work in 8 days, but this is not necessarily what most people can expect.
Another reason this is a hard question to answer is the different people have different expectations and also different definitions of the word “recovery.”
Here we’ll try to break down the road to recovery into phases, but just remember we all recover at our own pace, and while some people will recover a little faster than average, some will also be a little slower.
The first phase of “recovery” actually start before surgery. How prepared you are for surgery often influences your speed and degree of recovery.
- Range of motion: Patients with better range of motion (how well you can bend and straighten your knee) before surgery are often able to regain their motion back faster and better after surgery.
- Weight: Patients who maintain a healthy body weight often recover faster (and have fewer surgery related risks) compared to those who are overweight.
- Stamina: Those with better exercise tolerance who are in better physical shape, often recover faster than those who are not.
The next thing that everyone always wants to know is how long the surgery will take. The answer is generally around 90 minutes.
Hospital Phase: Most patients stay in the hospital two nights. Most patients have their first physical therapy session on the day of surgery! This usually entails standing up and taking a few steps. Getting out of bed on the day of surgery has been shown to expedite recovery. The next two days are focused on getting you ready to go home, which means walking longer distances, going up and down stairs, and learning how to take care of yourself with your new knee.
The first six weeks is the next phase and is the one in which there is the most swelling of the leg, feet, and ankles. The knee is somewhat tender and sore with weight bearing. The old arthritis pain is usually gone after two weeks, but the soreness from the surgery will depending upon the level of activity. You will most likely need a cane for indoor activities for 1-2 weeks and for outdoor activities for 4-6 weeks. There is no need to rush the rehabilitation time and there are no gold medals for getting off the cane sooner. It is critical during this time frame that you do not overload the leg and you should use the cane if you are having a significant limp.

The next phase lasts about 3-4 months and at this time most people are able to be off the cane and do recognize that they have some return of leg strength. The leg will still be sore at this time, sometimes in the thigh and sometimes in the groin and sometimes in the lateral knee, particularly if the leg is overloaded. There cannot be rigid guidelines for activity levels because each patient does differ. However, you need to use your common sense and determine what activities you can be doing at this three month time frame and not exceed them. For golf, patients can chip and putt at 2 weeks and begin swinging the club at 4-6 weeks and play the course with some breaks at 2-3 months. Many patients return to work sometime during this phase depending on their workload.

The final phase is the 6 month time frame at which time activities can be done all day long without having to rest and endurance capability is near normal. The difference in the strength of the leg between 3 months and 6 months will be recognized, particularly for those patients who are involved in any sporting activities. More vigorous sporting activities such as snow skiing, water skiing, beach volleyball, mountain hiking, and the like should really wait for 6 months because the leg strength is so much better at 6 months and the ability to perform these activities with strength is much easier.
Some patients will take up to a full year to regain their full strength and stamina and get rid of all of the soreness.
The most important thing you can do is listen to your body and recover at your own pace.
What is a hip replacement made of?
What are the parts of a hip replacement?
Despite close to 1 million hip replacements being performed in the United States every year, very few patients know the parts and materials that compose a hip replacement.
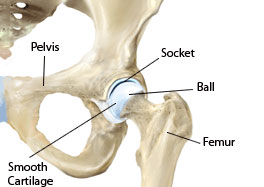
The hip is a ball and socket joint, and the goal of any hip replacement is to recreate the ball and socket. The socket (acetabulum) is part of the pelvic bones and the ball is the end part of the femur (thigh bone).
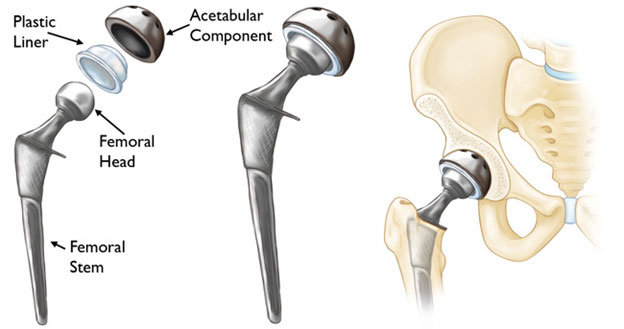
There are variations to every rule, but the standard hip replacement is made up of four different pieces: the femoral stem which sits inside the femur bone, the femoral head which recreates the ball of the ball and socket and sits on top of the femoral stem, the acetabular cup, which recreates the socket, and the acetabular liner that sits inside the acetabular cup to provide a new smooth joint surface.
What materials are the pieces made of?
Both the femoral stem and the acetabular cup are usually made from titanium and covered in a roughened surface that allows bone to grow into it, so that it eventually becomes incorporated into a patient’s body. Titanium is inert, which means that the body does not reject it. The femoral head has traditionally been made from a metal cobalt-chromium alloy, but more recently surgeons have been using ceramic heads to try to make hip replacements last longer. The liners have are made from a plastic called polyethylene, but metal and ceramic liners have both been tried and are occasionally still used. Older versions of this plastic had been known to wear out after 10-15 years, but the newer versions have been shown to last significantly longer, and in most cases last for the patient’s entire life.
What is a metal-on-metal hip replacement?
When a metal acetabular liner is used in combination with a metal cobalt chrome femoral head, this is called a metal-on-metal hip replacement (MoM). Initially the thought was that these MoM hips would never wear out and could replace the traditional metal liner and plastic ball joint, but it was discovered that these hips often released tiny metal particles that could cause aggressive reactions around the hip joint as well as problems throughout the body if these particles were absorbed into the blood stream. For these reasons metal on metal hips have mostly fallen out of favor.
What is a squeaking hip?
When a ceramic liner was used with a ceramic femoral head (ceramic-on-ceramic), it occasionally produced a very loud squeak, which patients found very annoying and, thus the ceramic liners also fell out of favor. When the two pieces of ceramic rubbed together very rarely one of the pieces of ceramic would shatter which would be a devastating problem. Both metal-on-metal and ceramic-on-ceramic designs tried to solve the problems caused by the older model plastic liners wearing out. Since the newer models of plastic liners have been shown to be so effective and last longer, the vast majority of hip replacements done today are with a ceramic or metal femoral head and a plastic acetabular liner.
What is the difference between a partial and total knee replacement: Which one is right for me?
One of the most common questions that I get asked is “What is the difference between a partial and a total knee replacement, and am I a candidate for one or the other?”
There is a second question that you must ask with this question which most patients don’t know to ask, and that is “Do you perform both operations?” Because if the answer to this question is “no” then your surgeon may not be offering you the operation that is best for you.
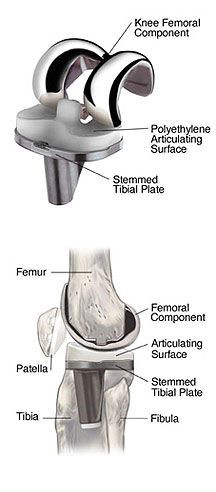
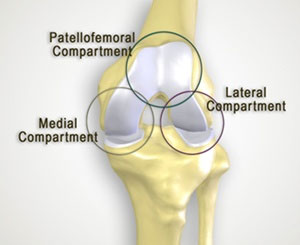
As with almost every question in orthopedics, it is important to understand some anatomy before the question can be answered. Although the knee is one joint composed of three bones, the femur (thigh bone), tibia (shin bone), and patella (knee cap), it is actually made of three distinct compartments. The three compartments are the medial (inside), lateral (outside) and patellofemoral (underneath the knee cap).
One more important piece of information that you need to know when discussing partial and total knee replacements is the definition of arthritis. Most people think that arthritis is something in the knee that we take out. In fact, it is just the opposite, arthritis is the generalized wearing away of the cartilage which acts as the cushioning in our joints. The most common type of arthritis is osteoarthritis, which occurs due to generalized wear and tear. Two other types of arthritis are post-traumatic arthritis, which is an injury to cartilage due to a traumatic event or distinct injury such as a broken bone, and inflammatory arthritis where the body’s own immune system mistakenly attacks its own joints.
So, back to our question, “What is the difference between a partial and a total knee replacement, and am I a candidate for one or the other?”
With our new knowledge, the answer becomes simple….
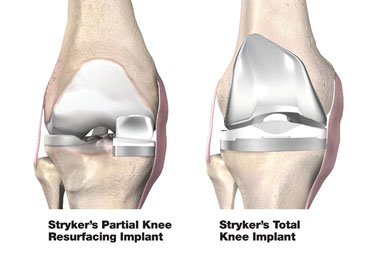
If you have arthritis that effects predominantly one compartment (see picture on the right below) of the knee that causes pain in that area and it does not response to conservative treatment (like rest, ice, medications, and injections), then you would be a candidate for a partial knee replacement, which selectively resurfaces only one compartment of the knee.
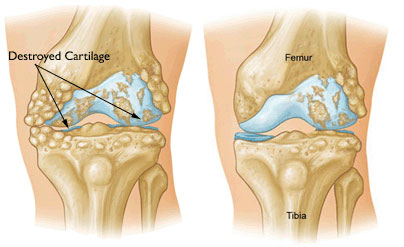
If you have arthritis that effects two or three compartments of the knee (see picture on the left above) and have not responded to conservative treatment, then a total knee replacement, which resurfaces all three compartments, is likely a better option.
A partial knee replacement is generally a smaller operation than a total knee replacement and has a slightly faster recovery and generally lower risks of complications such as infection and blood clots (although the risks for total knee replacement are generally quite low as well). The one major drawback to partial knee replacements when compared to total knee replacement is the risk of the non-resurfaced compartments wearing out. Since a total knee replacement resurfaces all compartments, this risk is not associated with total knee replacements. If a patient has a partial knee replacement and the other compartments wear out over time, then he or she would require another operation to convert the partial knee replacement into a total knee replacement (easier said than done).
Ultimately the goal of both surgeries is the same, to get rid of pain and return to back to being able to do the things that you weren’t able to do due to pain in your knee. Talk to your surgeon about which operation is the best choice for you. I am proud to offer both procedures to our patients.
Call today at 914-631-7777 to schedule an appointment and find out which procedure is right for you.
Lifelong physical activity increases bone density in men
Men have many reasons to add high-impact and resistance training to their exercise regimens; these reasons include building muscle and shedding fat. Now a researcher has determined another significant benefit to these activities: building bone mass. The study found that individuals who continuously participated in high-impact activities, such as jogging and tennis, during adolescence and young adulthood, had greater hip and lumbar spine bone mineral density than those who did not.
Source: Science Daily


