












All posts by hochfelder
Over-the-counter painkillers treated painful injuries just as well as opioids in new study
In a new study of patients who showed up to an emergency department with acute pain in their shoulders, arms, hips or legs, researchers found that a cocktail of two non-addictive, over-the-counter drugs relieved pain just as well as — and maybe just a little better than — a trio of opioid pain medications widely prescribed under such circumstances.
Source: Los Angeles Times
Morbidly obese, nonobese patients experienced similar outcomes after revision THA
Morbidly obese patients who underwent aseptic revision total hip arthroplasty experienced similar complications, failures and clinical outcomes compared with nonobese patients, according to study results.
Source: Healio
Research finds decrease in opioid use among patients recovering from hip and knee replacement
Opioid use in patients recovering from hip and knee replacement decreased by one-third between 2006 and 2014, reflecting success in efforts to promote a multimodal approach to pain management (using a variety of methods to manage pain) rather than using opioids alone, reveals new research being presented at the ANESTHESIOLOGY® 2017 annual meeting.
Source: News-medical.net
Obesity to Blame for Epidemic of Knee Problems
Need another reason to keep your weight under control?
Excess weight can cause dislocation of your knee and may even lead to a complication that results in amputation of your leg.
A new study attributes a surge in dislocated knees to the U.S. obesity epidemic.
Source: WebMD
Rule out infection, adverse local tissue reaction during investigation of THA instability
When a hip becomes unstable after total hip arthroplasty, the orthopedic surgeon should investigate it with a history and physical, appropriate imaging and laboratory tests prior to any surgery to remove the hip anteversion or revise the prosthesis, according to a presenter.
Source: Healio
What is a hairline fracture?
Hairline or stress fractures are tiny cracks on a bone that often develop in the foot or lower leg. It is common for hairline fractures to occur as a result of sports that involve repetitive jumping or running.
Source: Medical News Today
Will My New Hip or Knee Last Forever?
Maybe.
I have patients in my office every weeks or so that had their hip or knee replaced 10-15 years ago and their doctor told them that they would have to have it redone in 10-15 years. I ask these patients “Does your hip or knee hurt?” and the answer is usually “No”. I take X-rays that show a good looking knee or hip replacement, and their exam is normal. I then get to deliver the good news that the knee or hip looks good and does not need to be redone, and in fact likely will never need to be redone.

The moral of the story is that we have found that hip and knee replacements are lasting longer than we ever thought possible. Of course there are always risks to any surgery and infection (in most patients less than one half of a percent chance) or premature loosening (also less than one percent chance) can lead to patients needing to have their knee or hip prematurely redone. However; barring any of these very rare risks, most patient’s new hips and knees will last them forever.
Many of the old problems that led to knees and hips needing to be redone such as inferior plastic materials that would wear out early, faulty cementing techniques, poor implant design and less accurate implantation techniques have been solved or at least minimized.

Some young patients worry that they are too young to have a hip or knee replacement. To them I say that we have data on young patients who had hips and knees replaced, and 35 years later, 78% of these people still had their original replacement! The knees and hips done 35 years ago were done with the above mentioned inferior techniques and with inferior technology, so we can only believe that today’s knees and hips will last even longer.
With the newer techniques and technology and the new data that we have today, we now tell patients to expect their new joint to last forever. Even young patients who were once told that they were too young and needed to wait and suffer until they were old enough are now encouraged to do the right thing, have the surgery that they need, and get back to living their life with a new knee or hip.
What is “hip arthroscopy” and is it right for me?
As with most things in medicine, an understanding of anatomy makes both problems and solutions a lot easier to understand. The hip is a ball and socket joint. The ball part is the upper end of the femur or thighbone and the socket is part of the pelvis called the acetabulum.
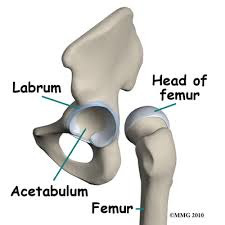
The end of each bone is covered in a shinny white material called cartilage, which acts as a shock absorber. There is another piece of cartilage that looks like a white gummy worm and wraps around the socket called the labrum. The labrum’s job is both to increase the surface area of the socket to allow for increased range of motion and also to help create a watertight seal, which assists in creating a stable joint.
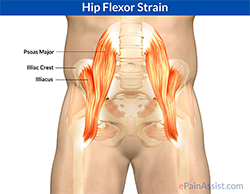
There area also numerous muscles and tendons that cross the hip joint such as the iliopsoas (hip flexor), which crosses right in front of the hip joint. The gluteus medius and minimus (hip abductors), which are on the side of the hip and attach to the big bump on our side act to move the leg out to the side and prevent us from toppling over when we walk. There are also little fluid filled sacks called bursa, which act as cushions, one of which is found right over the bump on the side of the hip, and another one sitting right on the hip flexor.
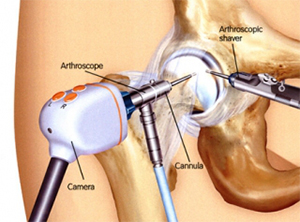
So now that we understand the anatomy a little better, we can now answer the first question. A hip arthroscopy is an outpatient procedure where a camera and small instruments are inserted into the hip through two to four small incisions on the front and outer thigh. Each incision usually requires only 1 or 2 stiches. Recovery from a hip arthroscopy depends a lot on what is done and can vary greatly from person to person. Often patients are on crutches for 2-4 weeks and do physical therapy for at least two months. Full recovery from a hip arthroscopy can take anywhere from 6 months to a year. Despite being a minimally invasive outpatient procedure, quite a lot can actually be done.
Femoroacetabular Impingement and Labral Tears
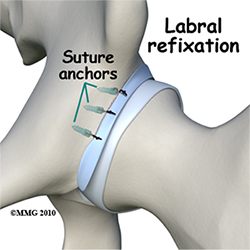
This is by far the most common indication for hip arthroscopy today. The labrum can tear from either an acute injury, overuse, or due to a specific anatomical variation that causes excess bone or a bone spur on the femur (thighbone) to impinge pinch on excess on the acetabulum (hip socket) when the hip is flexed up. This last cause is called femoroacetabular impingement. If the labrum tears from an acute injury or overuse, it can simply be repaired back into place by anchoring it back to the socket. If the labrum tears due to femoroacetabular impingement, then the excess bone on the thigh bone or hip socket must be shaved down and moved in order to prevent the problem from recurring.
Cartilage Problems
The absence of cartilage in a joint is called arthritis. Patients with complete loss of cartilage usually cannot be treated with arthroscopy and are usually best treated by joint replacement. However; the very early stages of arthritis sometimes manifest as small defects (like a pothole) in cartilage that can be addressed by various arthroscopic techniques.
Loose Bodies
Occasionally a piece of cartilage will break off and get trapped in the joint like a pebble. These can be removed arthroscopically.
Iliopsoas Tendon (Hipflexor) Problems
The hip flexor can be a nagging source of pain for some patients. Whether it is due to overuse, an acute injury, or even a mal positioned hip replacement, a chronic irritation of the hip flexor is sometimes treated by arthroscopically releasing it. This can sometimes lead to about 15% loss of power in hip flexion, which is why arthroscopic release is usually a last resort.
Abductor tears and bursitis
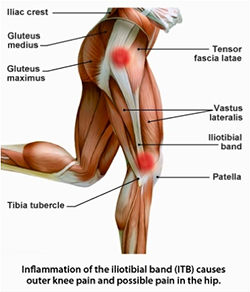
The muscles on the side of the hip and sometimes tear similar to the rotator cuff muscles in the shoulder. Partial tears can often be treated without surgery, but large full thickness tears sometimes require surgery to anchor the tendons of these muscles back down to bone. Sitting right on top of these muscles is a bursa called the trochanteric bursa. Trochanteric bursitis (inflammation or irritation of this bursa) can be a very difficult problem to treat and can be treated with excision of the bursa.
Study to evaluate outcomes of different hip replacement techniques using mobile gait analysis system
Researchers at Hospital for Special Surgery (HSS) have launched a pilot study using a portable gait analysis mat to determine early outcomes of several different hip replacement techniques. Gait analysis provides information about the way an individual walks.
Source: News Medical Net
Large variation found in 3-D UKA alignment analysis for femoral, tibial components
Recently published results showed large variation in the rotational plane for both femoral and tibial components during 3-D unicompartmental knee arthroplasty component alignment analysis in the standing position, suggesting the importance of component positioning.
Source: Healio


